

Translate this page into:
Multidetector computerized tomography in diagnosis and preoperative workup of fetus in fetu: A case series
Corresponding author: Prof. Amit Nandan Dhar Dwivedi, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India. amitnandan21@yahoo.com
-
Received: ,
Accepted: ,
How to cite this article: Dwivedi AND, Gupta PN. Multidetector computerized tomography in diagnosis and preoperative workup of fetus in fetu: A case series. Future Health. 2024;2:58–60. doi: 10.25259/FH_1_2024
Abstract
Fetus in fetu is a rare disorder with a reported incidence of 1 in 500,000 live births, with only 78 cases reported so far. The most common presentation is abdominal mass in a newborn or infant; however, presentation in later life is also possible. Early detection is by ultrasonography. Computerized tomography is rarely used. However, computerized tomography gives an excellent overview of anatomical information and its exact relation with the surrounding viscera. The present case series is an attempt to highlight the role of cross-sectional imaging in the pre- and post-operative management of this rare disorder.
Keywords
Fetus in Fetu
Teratoma
Computerised Tomography

INTRODUCTION
Fetus in fetu hypothetically represents a monozygotic diamniotic twin that implants and grows as a parasite within the body of its normal karyotypically identical sibling. The theory of highly differentiated teratoma is also believed by many authors.1 The oldest patient reported to date is 29 years old.2 The mass is usually located in the upper retroperitoneum in most of the cases. Fetus in fetu has been reported to occur in other locations, such as the cranium,3 scrotum,4 and the oral cavity.5 In most of the cases, the presence of a single parasitic twin is noted; however, cases of as many as five multiple implanted twins have been observed. Radiographs act as the first indicators of the disease in case of infants presenting with a lumped abdomen. Other modalities like ultrasound, Doppler, and cross-sectional imaging like computed tomography (CT) and magnetic resonance imaging (MRI) help in further confirming the diagnosis and preparing a road map for pre- and post-operative management.
The present case series highlights the imaging findings of a CT scan and its invaluable role in providing exact anatomical landmarks and relation with the host. It proves to be a very useful tool in preoperative management of such cases.
CASE SERIES
Case-1
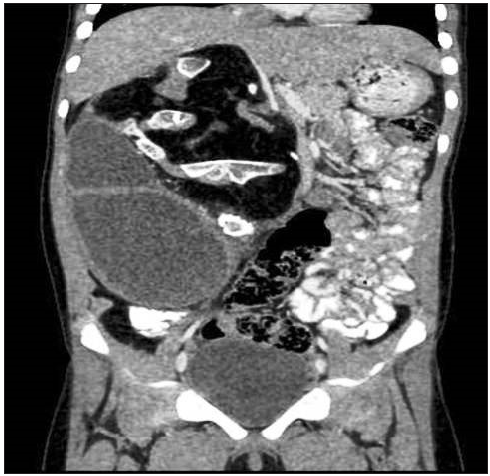
A two-month-old girl child was presented in the pediatric surgery department with complaints of a lump abdomen with stable vitals and accepting oral feeds. On examination, the mass was non tender. The child was sent to the Department of Radiology for a detailed workup. Plain radiographs suggested long bones within the fetal abdomen. Differential diagnosis included a well-differentiated teratoma or fetus in fetu. To assess the presence of vascularity and further anatomical characterization, an ultrasound sonography (USG) of the abdomen was performed. A detailed ultrasound revealed a large inhomogeneous mass in the retroperitoneum containing both fat and calcification. A CT scan was done to obtain detailed anatomical information and characterization of the anomaly. CT scan revealed a large mass containing a large area of fat and fluid with partially formed spinal curvatures and a well-formed knee joint showing femoral condyle, tibial plateau, and patella. Skull bones were not seen [Figure 1]. No encasement of any major organ was noted; however, gross displacement of the visceral organ without any obvious sign of infiltration was seen. Surgical exploration showed a well-formed fetus covered with skin and lanugo. There were well-formed lower and upper limbs, a spinal canal, and acranic brain parenchyma. Anal dimple was noted, however, genitalia was not developed [Figure 2]. The patient had an uneventful postoperative course following the excision of the fetus in fetu.

- CT scan coronal view bone window showing well-formed femur with patella and tibia forming knee joint contained within well-defined sac along with fat and soft tissue in left hypochondrium and left lumbar region.

- Postoperative specimen showing soft tissue mass with well-formed skin with lanugo, anal pit, and limbs. Brain parenchyma without calvaria is also noted.
Case-2
A two-year-old girl was presented with a smooth non tender lump in the abdomen. The child was active and had normal developmental milestones. The parents observed a mild increase in mass within three weeks of birth. Similar protocols were followed as in a previous case and subsequently CT scan was performed. CT scan showed a well-formed area of fat and fluid in the retroperitoneal space in the right lumbar space. A well-formed ankle and tarsal bones were noted, but an ipsilateral kidney was not seen. No spinal canal could be delineated. There was no evidence of upper limbs and skull bones [Figure 3]. Differential of well-differentiated teratoma and fetus in fetu was kept in this particular case. The patient underwent surgical removal of the mass. There was a good correlation of the mass on gross inspection with the preoperative information obtained from the CT scan. Useful information was obtained from virtually reconstructed images during post-processing of images. Gross examination after surgical removal of 1.5 kg parasitic twin showed a well-formed fetus with well-formed appendicular skeleton and skin covering. Anal dimple was noted, but genitalia were poorly developed. Both cases showed a cystic fluid-filled cavity that represented acranic brain parenchyma. Post-operative recovery was good, and the patient was discharged.
- CT scan coronal view bone window showing well-formed ankle joint and metatarsal bones in another case in right hypochondrium.
CT scan proved to be an excellent modality to delineate fat planes, determining the course of further management and ruling out any malignant transformation and associated anomalies.
DISCUSSION
Fetus in fetu clinically presents as a lump in the abdomen (70%), mainly in the upper retroperitoneum.6 Single parasitic fetus is the commonest presentation (88%). The present fetal size was approximately 13 cm x 10 cm. The fetal weight varies between 1.2 kg and 1.8 kg, and it was 1.5 kg in both cases. Cross-sectional imaging helps to rule out all common causes of lump abdomen, except teratoma and fetus in fetu. The presence of a vertebral axis and identification of limbs is characteristic of fetus in fetu and excludes the diagnosis of teratoma.7 The organs demonstrated are, namely, spine in 91%, limbs in 82.5%, CNS in 55.8%, GIT in 45%, vessels in 40%, and GUT in 26.5% cases, respectively.8 The vertebral column is an important clue that suggests the formation of a notochord, which is an advanced primitive streak stage. A noncalcified vertebral column invisible on a radiograph or a CT scan or its total absence (9%) does not exclude the diagnosis of the fetus in fetu.9 In our study, the spinal canal was not identified on the cross-sectional imaging in one of the cases, which turned out to be a fetus in fetu on postoperative gross examination. Most of these fetuses are anencephalic,1 which was also observed in both our cases. Fetus in fetu gets its blood supply from the rich vascular plexus around the well-formed cyst wall. Vascular pedicle is unusual and observed in large growing masses with delayed presentation.10 Malignant transformation is rare in the fetus in fetu, and only one case has been reported in literature.11 However, it may increase in size and can cause local mass effects in terms of hemorrhage. The role of imaging is diagnostic, and a CT scan is a valuable modality showing round or tubular fat collection around central bony structures.12 Surgical excision is the treatment of choice, and gross examination confirms the diagnosis. Our pre-operative and postoperative findings were similar to cases reported earlier in the literature.
CONCLUSION
Fetus in fetu is a rare pathological condition, and CT scan findings play a vital role in diagnosing this anomalous embryogenic disorder in monozygotic diamniotic twins. It provides important anatomical information for pre- and postoperative management.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent is not required as patient’s identity is not disclosed or compromised.
Financial support and sponsorship
Nil
Conflicts of interest
There are no conflicts of interest
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Fetus in fetu: a case report and literature review. Pediatrics. 2000;105:1335-44.
- [CrossRef] [PubMed] [Google Scholar]
- Dysphagia caused by a fetus in fetu in a 29 year old man. Am.Thorac. Surg. 2001;71:1338-41.
- [Google Scholar]
- A cerebral tumor containing five human fetuses: a case of fetus in fetu. Anat Rec. 1950;106:141-65.
- [CrossRef] [PubMed] [Google Scholar]
- Fetus in fetu located in the scrotal sac of a newborn infant: a case report. J Urol. 1972;107:506-8.
- [CrossRef] [PubMed] [Google Scholar]
- Fetus in fetu or giant epignathus protruding from the mouth. J Pediatr Surg. 1992;27:1493-5.
- [CrossRef] [PubMed] [Google Scholar]
- Postnatal growth of fetus in fetu. Pediatr Radiol. 1993;23:411-2.
- [CrossRef] [PubMed] [Google Scholar]
- The borderland of embryology and pathology (2nd ed). Washington DC: Butterworth; 1962. p. :442-62.
- Fetus in fetu or a re1troperitoneal teratoma--a controversy revisited. A case report and review of literature. Indian J Cancer. 1997;34:179-81.
- [PubMed] [Google Scholar]
- Fetus in fetu: CT appearance report. Radiology. 2000;214:735-7.
- [CrossRef] [PubMed] [Google Scholar]




