

Translate this page into:
Popliteal artery pseudoaneurysm following arthroscopic lateral meniscus root repair
*Corresponding author: Dr. Rajiv Kaul, Department of Orthopaedics, Military Hospital Dehradun, Dehradun, India. drrajivkaul@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Iqbal MS, Sood M, Kaul R. Popliteal artery pseudoaneurysm following arthroscopic lateral meniscus root repair. Future Health. doi: 10.25259/FH_3_2025
Abstract
Pseudoaneurysms of the popliteal artery can lead to serious complications such as hemorrhage following rupture of the pseudoaneurysm, venous compression by a large pseudoaneurysm, and thrombosis or embolization leading to limb ischemia, and a possibility of limb loss. We present and discuss a case of pseudoaneurysm of the popliteal artery following arthroscopic lateral meniscus root repair in a young male and the treatment strategies for the same.
Keywords
Arthroscopy
Meniscal root repair
Popliteal
Pseudoaneurysm
Self-resolving

INTRODUCTION
The anatomic proximity of the popliteal artery to the posterior capsule of the knee makes it vulnerable to injury during knee surgery.1 Although the risk to the popliteal artery due to different arthroscopic procedures has been researched in detail by various cadaveric studies, the occurrence in clinical practice is extremely rare.2 We highlight a case of a popliteal artery pseudoaneurysm following a lateral meniscus root repair in the early post-operative period in a young athlete.
CASE REPORT
A 31-year-old male athlete sustained a twisting injury to his left knee and presented to us a year later with pain and instability in the affected region. Clinical examination revealed a positive McMurray’s and Lachman test; magnetic resonance imaging (MRI) revealed a complete anterior cruciate ligament (ACL) tear with a complex tear of the posterior horn of the lateral meniscus.
Arthroscopic findings
Intra-operatively, the ACL was completely torn from the femoral attachment, and the lateral meniscus had a complex tear extending into the root. In addition to standard medial and lateral parapatellar arthroscopic portals, a supra-meniscal portal was made to gain access to the lateral meniscus root, which provided a good trajectory for root repair. The lateral meniscus body tear was repaired using two FAST-FIX 360 (Smith & Nephew, Watford, UK) sutures, while the root tear was repaired using the transtibial pullout technique with FIRSTPASS mini suture passer (Smith & Nephew, Tennessee, USA) and FibreWire (Arthrex, Naples, USA). ACL reconstruction was done using the ipsilateral quadrupled semitendinosus graft with a fixation on the femoral side using an adjustable loop EndoButton (Smith & Nephew, Watford, UK) and on the tibial side using a Bioscrew.
Post-operative period
On the 4th post-operative day, the patient developed a mild fever with tense swelling in the operated knee. There was no associated swelling in the calf. Distal pulses were palpable bilaterally. Presuming it to be a consequence of overzealous physiotherapy, we resorted to conservative management in the form of oral analgesics and cryotherapy. However, the swelling continued to increase over the next two days, which prompted us to perform a diagnostic synovial fluid aspiration of the knee. The aspirate was approximately 150 mL in quantity and notably had blood. The clinical indicators of progressively increasing pain and swelling pointed towards a possible vascular mishap, such as a popliteal vessel tear or fistula. This prompted us to perform an urgent CT angiogram, which revealed a 5 mm pseudoaneurysm in the short segment of the left popliteal artery along the medial wall, without any extravasation of contrast into the surrounding tissues [Figure 1].
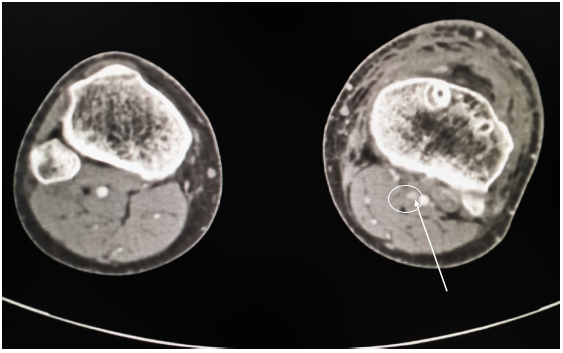
- Post-operative CT angiogram, axial section showing a 5 mm pseudoaneurysm in the short segment of the left popliteal artery (white arrow and circle). The white dot within the circle represents the area of the pseudo-aneurysm. CT: Computed tomography.
Management and follow-up
Vascular-surgeon consultation was obtained, and considering the size of the lesion, the patient was managed with expectant observation for the pseudoaneurysm and the standard post-ACL reconstruction rehabilitation was de-escalated to continuous passive motion (CPM) for two weeks. The swelling in the knee subsided following the aspiration. The patient was reviewed after two months with a repeat CT angiogram, which showed a complete resolution of the pseudoaneurysm [Figure 2]. Six months later, the patient was reviewed again and had a fully functional and pain-free operated limb.
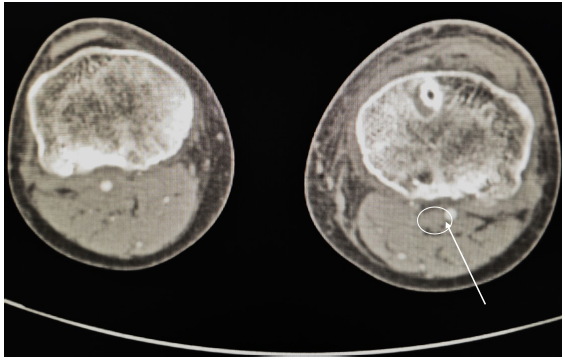
- Follow-up CT angiogram at 2 months, axial section showing complete resolution of the pseudoaneurysm (encircled). White arrow and circle represents the area of the resolved aneurysm. CT: Computed tomography.
DISCUSSION
The occurrence of a popliteal artery injury during knee arthroscopy is not always recognizable. Pseudoaneurysms, or false aneurysms, contain a vessel-derived hematoma enveloped by partial elements of the arterial wall, fibrous tissue, and neighboring stroma, with an incidence rate of 0.05-4%.3 The most affected arteries are the popliteal (45.83%) and the inferomedial genicular arteries (20.83%).4,5 The risk of injury to the popliteal artery is related to its close anatomic location to the posterior capsule and its movement during knee flexion.6 The artery is separated from the joint capsule by minimal fat, which may be why it is so frequently affected.3 As the posterior corners of the knee are difficult to view during arthroscopy, immediate viewing of an iatrogenic bleed is almost impossible. Hence, such injuries are often recognized late, and it is crucial to examine the circulation in the limb after any arthroscopic surgery. Although our case presented with features of normal distal circulation, we emphasize the importance of keeping a high suspicion of vascular events, in cases with normal distal circulation.
Cadaveric studies have reported that operating on the posterior horn of the lateral and not the medial meniscus places the popliteal vessels at risk.2 Massey et al. reported that the mean distances from the tip of the needle to the popliteal neurovascular bundle in a lateral meniscal repair from anteromedial, anterolateral, and trans-patellar approaches were 6.9, 3.1, and 6.5 mm respectively.7 Al-Fayyadh et al. found that utilizing the anteromedial portal to repair tears located 15 mm on the lateral meniscus’ posterior horn will be very safe, as the portal’s trajectory does not head towards the artery.8 Conversely, repairing the posterior horn of the lateral meniscus 5–10 mm away from the posterior root, utilizing the anterolateral arthroscopic portal, places the popliteal artery at risk. Precautionary measures while performing a lateral meniscus root repair via an anterolateral working portal include the use of a curved needle directed away from the artery and limiting the depth of penetration of the inserter needle.
Due to the rarity of these lesions, there is a paucity of data to guide management. Most pseudoaneurysms, less than 2-3 cm, may be treated conservatively with surveillance duplex scanning until they resolve spontaneously.2 For symptomatic lesions larger than 3 cm, treatment options include ultrasound-guided compression, ultrasound-guided injection of thrombin, therapeutic embolization, endovascular stenting, and open repair using interposition vein grafts.2
The most devastating complication of a pseudoaneurysm is rupture, which is typically seen in the common femoral artery;3 risk factors include the presence of peripheral vascular disease, elevated plasma liver enzymes, and advanced age.2
For diagnostic aids, we advocate the use of a CT angiogram vis-a-vis Color Doppler Flow Imaging (CDFI) since a CT Angiogram replicates the entire arterial anatomy within minutes, giving precise information about the exact location and size of the lesion.9 However, it bears the risk of radiation-associated hazards. CDFI is limited due to a wide inter-observer variability, longer examination time, and limited reproducibility.
CONCLUSION
This report demonstrates the importance of having a high index of suspicion for popliteal artery aneurysm/pseudoaneurysms following a lateral meniscus root repair, which may be masked by hemarthrosis of the knee. Management of this condition requires a multi-disciplinary approach and periodic follow-up, which must include appropriate radiological investigations.
Author contributions
MSI: Conceptualising, data processing, article review; MS: Project administrator, article review; RK: Article writing and data processing.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
Patient’s consent not required as patients identity is not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of Artificial Intelligence (AI)-Assisted Technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
References
- Popliteal pseudoaneurysm and arteriovenous fistula after arthroscopic meniscectomy. Arthroscopy. 2001;17:E1.
- [CrossRef] [PubMed] [Google Scholar]
- All-inside lateral meniscal repair via anterolateral portal increases risk of vascular injury: A cadaveric study. Arthroscopy. 2020;36:225-32.
- [CrossRef] [PubMed] [Google Scholar]
- Delayed pseudoaneurysm of the popliteal artery following ACL reconstruction. Orthopedics. 2015;38:e543-6.
- [CrossRef] [PubMed] [Google Scholar]
- Pseudoaneurysm after arthroscopic procedure in the knee. Rev Bras Ortop. 2015;50:131-5.
- [CrossRef] [PubMed] [PubMed Central] [Google Scholar]
- Pseudoaneurysm as a complication of knee arthroscopy. Arthroscopy. 1997;13:644-5.
- [CrossRef] [PubMed] [Google Scholar]
- The location of the popliteal artery in extension and 90 degree knee flexion measured on MRI. Knee. 2009;16:143-8.
- [CrossRef] [PubMed] [Google Scholar]
- Proximity of the neurovascular bundle during posterior-lateral meniscal repair: A comparison of the transpatellar, anteromedial, and anterolateral portals. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2019;35:1557-64.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluating the risk of popliteal artery injury in the all-inside meniscus repair based on the location of posterior meniscal lesions. J Orthop Surg (Hong Kong). 2019;27:2309499019828552.
- [CrossRef] [PubMed] [Google Scholar]
- Segmental comparison of peripheral arteries by doppler ultrasound and CT angiography. J Clin Diagn Res. 2016;10:TC12-6.
- [CrossRef] [PubMed] [Google Scholar]




